Designing for Patient Flow in a Multi-Chair Clinic

The Foundation: Strategic Operatory Planning
An efficient clinic is built on a foundation of intelligent spatial design. Before considering advanced technologies or decor, the physical layout of your operatories dictates the rhythm of your practice. Poor planning at this stage creates friction that compounds with every patient, every day. A common pitfall I often see is clinics acquiring new chairs without a corresponding layout strategy, leading to cramped spaces that hinder staff and create bottlenecks.
The Dental Chair as the Epicenter: Footprint and Clearances
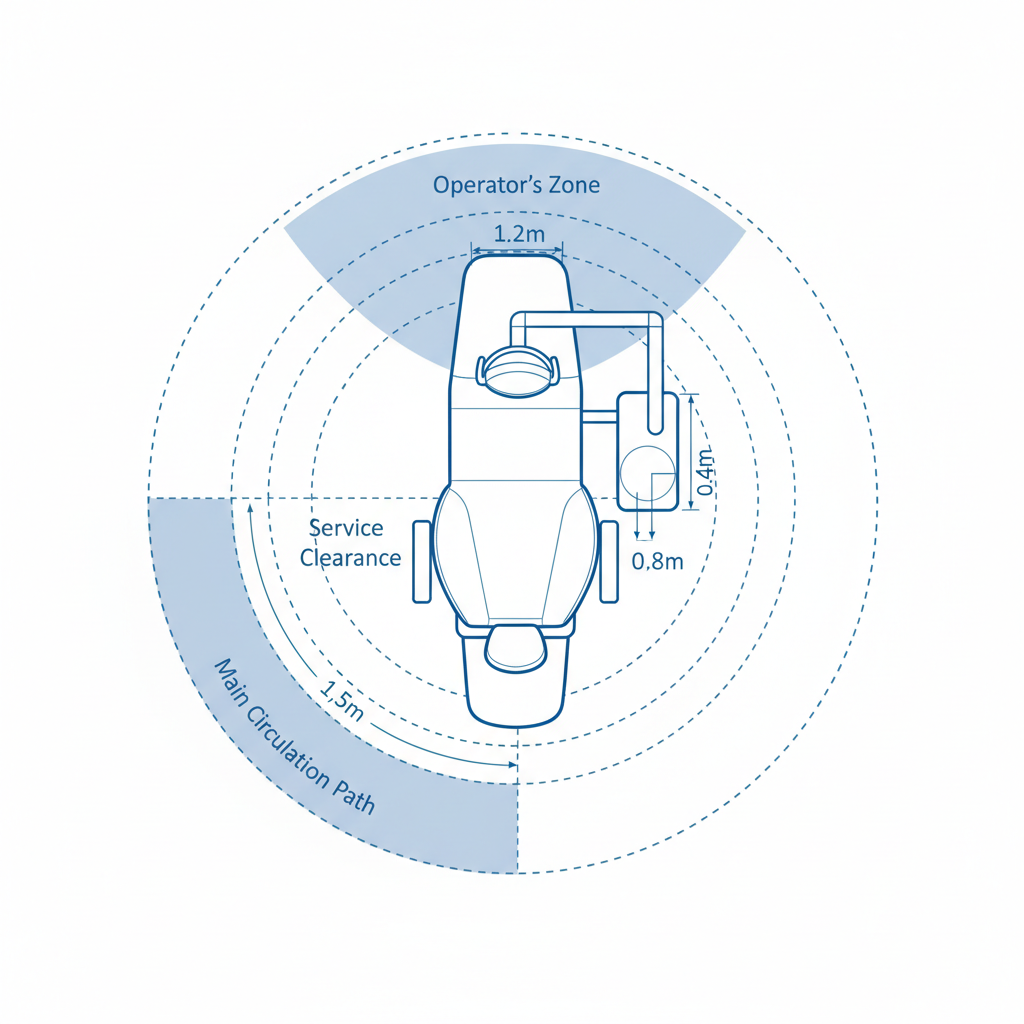
The dental chair is the heart of the operatory. Its placement determines not just patient comfort but the entire team’s ergonomic health and efficiency. Start by reserving a dedicated floor envelope of approximately 1.2 m × 1.8 m for each chair. This isn’t just for the chair itself, but for its full range of motion.
From there, plan your clearances. These are non-negotiable zones for safe and effective movement:
- Main Circulation Paths: Maintain a width of 1.2–1.5 meters for primary walkways. This allows two people to pass comfortably and prevents traffic jams, especially when moving mobile equipment or escorting patients.
- Service Clearances: The space around the chair where assistants work needs 0.6–1.0 meters. This allows them to access instruments and assist the operator without contorting their bodies or reaching awkwardly.
- Operator’s Zone: A critical but often overlooked space is the 1.2-meter clear zone directly behind the practitioner. I used to get persistent back and shoulder strain from twisting to reach rear-delivery units. Creating this dedicated zone allows for proper posture and direct access to essential equipment without compromising ergonomics.
Utility Routing: The Unseen Workflow Killer
A mistake I see far too often is underestimating the complexity of utility routing. Power, compressed air, suction, and data lines are the clinic’s circulatory system. Planning these routes as an afterthought is a recipe for disaster, often leading to exposed conduits, tripping hazards, and extremely expensive retrofitting that requires tearing up floors or walls.
Work with your architect and equipment supplier early to map these lines directly into the floor plans. Consider future needs as well. Adding one extra conduit pipe during initial construction is a minor cost, but adding it five years later can disrupt operations for weeks and cost ten times as much. This forward-thinking approach is essential for a scalable practice and aligns with the robust quality management systems outlined in standards like ISO 13485:2016, which emphasize controlled and well-documented infrastructure.
Debunking a Common Myth: “More Chairs Always Means More Revenue”
There is a pervasive myth in practice management that increasing the chair count directly translates to higher profits. In reality, adding chairs into a poorly designed space creates chaos, not efficiency. Without adequate circulation paths, sufficient sterilization capacity, and optimized scheduling, extra chairs simply lead to more staff collisions, longer patient wait times, and increased stress. The true metric of productivity is patient throughput per chair, which is a function of flow, not just capacity. A well-designed four-chair clinic can often outperform a cramped and chaotic six-chair one.
Optimizing Workflow Around the Chair
With the operatory footprint established, the next layer of design focuses on micro-workflows—the sequence of movements performed during treatment. Every second saved by eliminating unnecessary steps or awkward reaches multiplies across hundreds of appointments, boosting productivity and reducing staff fatigue.
The “Arm’s Length” Principle for Instrument Staging
Keep all frequently used instruments and consumables within a primary reach zone of 0.6 to 1.5 meters from the operator. This area—roughly an arm’s length plus a small step—is where instrument staging should occur. Forcing staff to constantly get up and walk to distant counters or cabinets wastes valuable time and increases the risk of cross-contamination. I found that using mobile carts and well-organized over-the-patient delivery systems was a game-changer. It kept everything I needed within reach, minimizing handoffs with my assistant and allowing me to stay focused on the patient.
Open vs. Closed Operatory Layouts
The decision between an open-bay or closed-room design has significant implications for patient flow, privacy, and equipment costs. Neither is universally “better”; the right choice depends on your practice’s specialty and patient demographic.
| Feature | Open-Bay Layout | Closed-Room Layout |
|---|---|---|
| Patient Flow | Excellent for high-volume, quick procedures (e.g., orthodontics, pediatric dentistry). Allows easy staff movement between chairs. | Better for longer, more complex procedures. Patient transport is more linear and defined. |
| Patient Privacy | Limited. Acoustic and visual privacy is minimal, which can be a concern for sensitive treatments. | High. Walls and a door provide complete confidentiality, which is often expected for adult restorative or surgical care. |
| Equipment Utilization | Allows for sharing of mobile equipment like X-ray units or specialized carts between multiple chairs, reducing capital investment. | Requires dedicated equipment for each room, increasing upfront costs but ensuring availability. |
| Noise & Infection Control | Aerosols and noise can travel more freely between stations, requiring robust HVAC and suction systems. | Provides superior containment of noise and aerosols, simplifying infection control within the room. |
Scaling Operations: Centralized Support Systems
A multi-chair clinic is more than a collection of operatories. Its efficiency hinges on centralized support systems that serve all chairs seamlessly. As you scale, these shared resources become critical to preventing bottlenecks.
The Sterilization Hub: Ratios and Compliant Workflow
The sterilization and instrument processing area is the engine room of the clinic. A poorly designed sterilization bay will bring the entire practice to a standstill. As a rule of thumb, plan for one well-equipped sterilization bay for every 3–5 operatories. This ratio can vary based on procedure complexity, but it provides a solid starting point for capacity planning.
An efficient sterilization workflow is linear: it should have clearly designated zones for receiving contaminated instruments, cleaning, packaging, sterilizing, and storing. This one-way flow prevents cross-contamination and is a core principle of medical device regulations like the FDA’s 21 CFR Part 820. Also, designate a separate, clearly marked “quarantine” space for failed or damaged instruments to ensure they are not accidentally returned to service.

Reception and Wayfinding: Managing First Impressions
Bottlenecks often start at the front door. Overcrowding the reception area or placing it too close to the clinical zone creates a confluence of patient traffic, noise, and administrative chatter that spills into the treatment area. Design a reception space that is physically and acoustically separate from the operatories.
A simple but effective adaptation is to create a single, visible “wayfinding spine”—a main corridor from which all patient areas (reception, operatories, restrooms) are clearly visible and accessible. This reduces patient anxiety and minimizes the need for staff to give directions, freeing them to focus on clinical tasks.
Streamlining Appointments with Smart Scheduling
Even the most perfect physical layout can be defeated by a chaotic schedule. In a multi-chair environment, the schedule is the primary tool for directing patient flow.
Clinic Flow Efficiency Checklist
Use this checklist to audit your current patient flow and identify areas for improvement:
- Defined Clearances: Are circulation paths around each chair at least 1.2 meters wide?
- Ergonomic Reach: Are primary instruments and supplies staged within a 0.6–1.5 meter reach of the operator?
- Utility Access: Are utility connections (air, water, suction) located for easy access without creating tripping hazards?
- Centralized Sterilization: Is there a clear, one-way workflow from “dirty” to “clean” in your sterilization area?
- Staggered Scheduling: Are appointment start times offset by 10–15 minutes to prevent patient arrival clusters?
- Realistic Buffers: Do you allocate adequate turnover time between appointments (e.g., 10–15 minutes for hygiene, 20–40 for restorative)?
- Decongested Reception: Is the waiting area sufficiently separated from the clinical operatories to reduce noise and traffic interference?
- Clear Wayfinding: Can a new patient easily navigate from the entrance to the operatory and exit without confusion?
The Power of Staggered Starts and Turnover Buffers
Simultaneously starting all appointments at the top of the hour is a common scheduling mistake that guarantees hallway congestion. Instead, implement staggered starts with 10–15 minute offsets between chairs. This smooths out the arrival and departure of patients.
Equally important is building realistic turnover buffers into the schedule. A hygiene appointment might only require a 10–15 minute buffer for room cleaning and setup. However, a complex restorative or surgical procedure could require 20–40 minutes. Accurately budgeting this time prevents the entire day’s schedule from falling behind and reduces stress on the clinical team.
Wrapping Up: Key Takeaways for a High-Efficiency Clinic
Designing an effective multi-chair clinic is a study in workflow engineering. Success is not about packing in as many chairs as possible, but about creating a system where patients and staff can move with purpose and without friction. By focusing on a chair-centric layout with proper clearances, planning for utility needs from day one, optimizing the workflow within each operatory, and implementing smart scheduling, you build a resilient practice that is productive, safe, and scalable. This focus on operational excellence is a key differentiator in a competitive dental market, as noted by industry analyses from firms like Frost & Sullivan.
Frequently Asked Questions (FAQ)
What is the minimum recommended clearance around a dental chair?
For main circulation paths, a width of 1.2–1.5 meters is recommended. For the assistant’s working area around the chair, allow for 0.6–1.0 meters. Crucially, a 1.2-meter clear zone should be maintained behind the operator to ensure proper posture and equipment access.
How many sterilization bays do I need for a multi-chair clinic?
A general guideline is to have one fully equipped sterilization bay for every 3 to 5 dental chairs. This ratio ensures that instrument processing can keep up with the demands of the operatories without causing delays.
What is the most common layout mistake that hurts patient flow?
One of the most common and costly mistakes is underestimating the routing for utilities like power, compressed air, and suction. Planning this after the main layout is finalized often leads to expensive retrofitting, operational downtime, and compromised safety.
Disclaimer: This article is for informational purposes only and does not constitute professional architectural, engineering, or clinical advice. Clinic design should be undertaken in consultation with qualified professionals and in compliance with all local building codes and healthcare regulations.
References
About the Author




