 Skip to content
Skip to content Open vs. Closed Operatory: Which Layout Is Right?

Open vs. Closed Operatory: A Strategic Decision for Your Dental Practice
The layout of your dental operatories is one of the most foundational decisions a clinic owner or practice manager will make. It directly influences patient experience, staff workflow, infection control, and construction costs. Choosing between an open-concept design and private, enclosed rooms requires a careful analysis of your practice’s specific goals, patient demographics, and budget.
This guide provides a detailed, evidence-based comparison to help you determine which model best aligns with your clinical and business objectives. We will explore the critical factors that should guide your decision, moving beyond simple aesthetics to focus on long-term efficiency and patient trust.
Understanding the Core Models: Open-Bay vs. Enclosed Operatories
The first step is to understand the fundamental differences, advantages, and common applications of each layout.
The Open-Bay Operatory
An open-bay layout features multiple dental chairs arranged in a single, large space. Chairs may be separated by low partitions, cabinetry, or nothing at all. This model is frequently seen in pediatric dentistry, orthodontics, and dental schools. The primary advantage is maximizing space and fostering an environment of open communication and collaboration among staff. It allows for high visibility, which is a significant asset in training environments where supervisors need to oversee multiple procedures.
Practitioner experience shows that open bays can reliably increase chair utilization rates due to the ease of moving between patients and the shared use of resources.
The Enclosed Operatory
Enclosed, or private, operatories are individual rooms, each containing a single dental chair and sealed off by full-height walls and a door. This design is the standard for general, cosmetic, and surgical dentistry, where patient privacy and confidentiality are paramount. The enclosed space is superior for controlling noise, containing aerosols, and creating a calm, focused environment for both the patient and the practitioner. This separation is critical for discussing sensitive treatment plans and financial matters, building a foundation of trust.

A Comparative Framework for Your Decision
Choosing a layout involves a series of trade-offs. What you gain in one area, you may sacrifice in another. A common mistake is to focus solely on upfront cost without considering the long-term operational impacts. This table provides a structured comparison to guide your analysis.
| Feature | Open-Bay Layout | Enclosed Operatory | Key Considerations for Your Practice |
|---|---|---|---|
| Patient Privacy | Low. Conversations can be overheard, creating a lack of confidentiality. | High. Ensures patient privacy for consultations and procedures. | Essential for procedures requiring discretion (e.g., surgery, cosmetic dentistry). |
| Infection & Aerosol Control | Challenging. Aerosols can travel between stations, requiring enhanced HVAC and suction. | Superior. Containment of aerosols is much easier within a sealed room. | Enclosed rooms are better aligned with modern infection control standards, especially for aerosol-generating procedures. |
| Construction & Fit-Out Cost | Lower. Fewer walls, doors, and dedicated HVAC systems are needed. | Higher. Typically increases per-operatory construction costs by 25-40%. | A budget heuristic: the cost savings of an open bay can be offset by the need for acoustic treatments or enhanced ventilation. |
| Workflow & Collaboration | High. Staff can easily move between chairs and collaborate on cases. | Lower. Movement between rooms is less efficient; communication is more deliberate. | Ideal for training centers and pediatric clinics where team interaction is constant. |
| Space Efficiency (Footprint) | More efficient. Typically requires ~6–8 m² per chair. | Less efficient. Requires ~9–12 m² per chair to accommodate walls and doorways. | The right choice depends on your available square footage and desired number of chairs. |
| Flexibility & Reconfiguration | Moderate. Layout is fixed unless using modular furniture. | Low. Altering a hard-walled room is a major construction project. | Modular partitions can offer a middle ground, providing some privacy while allowing for future layout changes. |
Debunking a Common Myth: The “Cheaper” Open Bay
A pervasive myth is that open-bay layouts are always the most cost-effective solution. While the initial construction cost is lower, clinics often face unforeseen expenses to mitigate the design’s inherent drawbacks. The two most common patient complaints in open-concept clinics are noise and a lack of privacy. Addressing these issues with high-end acoustic ceiling tiles, sound-dampening panels, or partial-height glass partitions can significantly reduce the initial cost savings. When these remediation costs are factored in, a thoughtfully designed hybrid model or a phased build-out of enclosed rooms can prove more financially prudent over the long term.
Key Technical and Workflow Considerations
Beyond the high-level layout, the technical details of your operatory design are critical for daily function and long-term success. These insights are grounded in practitioner experience and regulatory awareness.
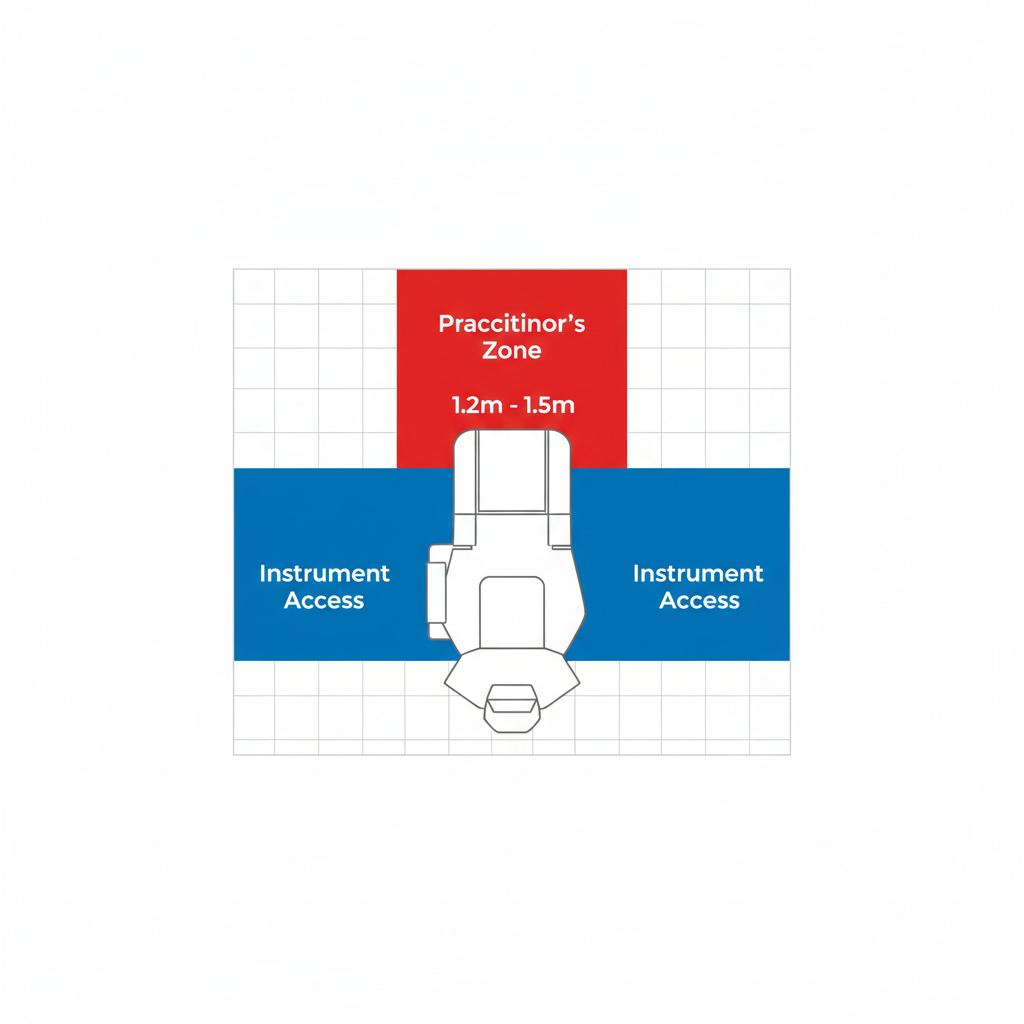
Spatial Planning and Clearances
One of the most frequent and costly planning mistakes is underestimating the space needed for an ergonomic workflow. Simply meeting minimum accessibility codes is not enough for an efficient clinical environment. Experienced practitioners report needing 1.2–1.5 meters of clearance behind the chair for unrestricted movement and 0.6–0.9 meters of lateral clearance for clear access to instruments and assistant carts. Failing to provide this space can lead to daily frustration, compromised posture, and an increased risk of workplace injury.
Aerosol Management and Infection Control
In the modern dental environment, robust infection control is non-negotiable. The ability to manage aerosols generated during procedures is a primary consideration. According to research highlighted by institutions like the National Institute of Dental and Craniofacial Research (NIDCR), controlling the spread of airborne particles is crucial. For enclosed operatories, a practical ventilation target is between 6 to 12 air changes per hour (ACH). In any layout, high-volume evacuation (HVE) is a key tool; studies published on platforms like PubMed demonstrate that placing the HVE suction tip within 40–60 cm of the oral cavity is highly effective at capturing aerosols at the source.
Utility Management and Future-Proofing
A forward-thinking design simplifies maintenance and future upgrades. Routing utility conduits—for air, water, suction, and data—within raised floors or dedicated service cavities behind walls is a best practice. This approach avoids the need to cut into concrete slabs or demolish walls for repairs or to accommodate new equipment, saving significant time and expense down the road. This aligns with the quality management principles outlined in standards like ISO 13485:2016, which emphasize the entire lifecycle of medical equipment.
Wrapping Up: Key Takeaways for Your Clinic
There is no single “best” operatory layout—only the one that is best for your practice. The decision between open-bay and enclosed designs hinges on a strategic balance between your budget, patient base, and clinical focus.
- Choose an open-bay layout if your primary focus is on orthodontics, pediatrics, or training, and your budget is the primary constraint. Be prepared to invest in acoustic and privacy enhancements to manage the inherent downsides.
- Choose an enclosed operatory if your practice performs a wide range of procedures, prioritizes patient privacy, and is focused on meeting the highest standards of infection control.
- Consider a hybrid model with modular partitions if you need a flexible solution that can adapt as your practice grows and evolves.
By grounding your decision in workflow efficiency, patient experience, and long-term operational costs, you can create a clinical environment that is productive, professional, and built for success.
Frequently Asked Questions (FAQ)
1. Can I convert from an open to a closed layout later?
Yes, this is possible, but the difficulty and cost depend on the initial design. Clinics that start with modular or partial partitions will find this process much simpler. Converting a true open bay with a hard-walled construction is a significant renovation project that requires careful planning around clinical downtime.
2. What is the biggest planning mistake clinics make?
Underestimating clearances. Many new clinics try to maximize the number of chairs by tightening the space around them, but this invariably leads to poor ergonomics, inefficient workflow, and staff frustration. Always prioritize adequate movement and access space over adding one more chair.
3. Are there specific regulatory requirements for operatory design?
Yes, dental operatory construction must adhere to local building codes, accessibility standards, and healthcare-specific regulations. Furthermore, the equipment and its installation must comply with medical device regulations, such as those from the FDA in the United States or CE marking requirements in Europe, to ensure safety and quality.
Disclaimer: This article is for informational purposes only and does not constitute professional architectural, legal, or medical advice. Clinic owners should consult with qualified architects, contractors, and regulatory experts to ensure their design complies with all applicable codes and standards.
References
About the Author





