Integrated Waterline Disinfection in Modern Dental Units

The Unseen Challenge in Dental Waterlines
Biofilm contamination in dental unit waterlines (DUWLs) represents a significant and persistent challenge to patient safety and regulatory compliance. While seemingly clean, the complex network of narrow-bore tubing inside a dental chair creates an ideal environment for microbial growth. This article explores the mechanics of integrated disinfection systems, their role in mitigating risks, and the essential protocols for ensuring their effectiveness.
At its core, a dental unit waterline is a network of small-diameter plastic tubing that transports water from a source—either a municipal line or a self-contained bottle—to high-speed handpieces, air/water syringes, and ultrasonic scalers. The very nature of this environment—with its low flow rates, intermittent periods of stagnation, and warm operating temperatures—makes it a fertile breeding ground for bacteria, fungi, and protozoa. These microorganisms attach to the inner surfaces of the tubing, forming a resilient, self-protective matrix known as biofilm.

Understanding Biofilm: A Persistent Threat
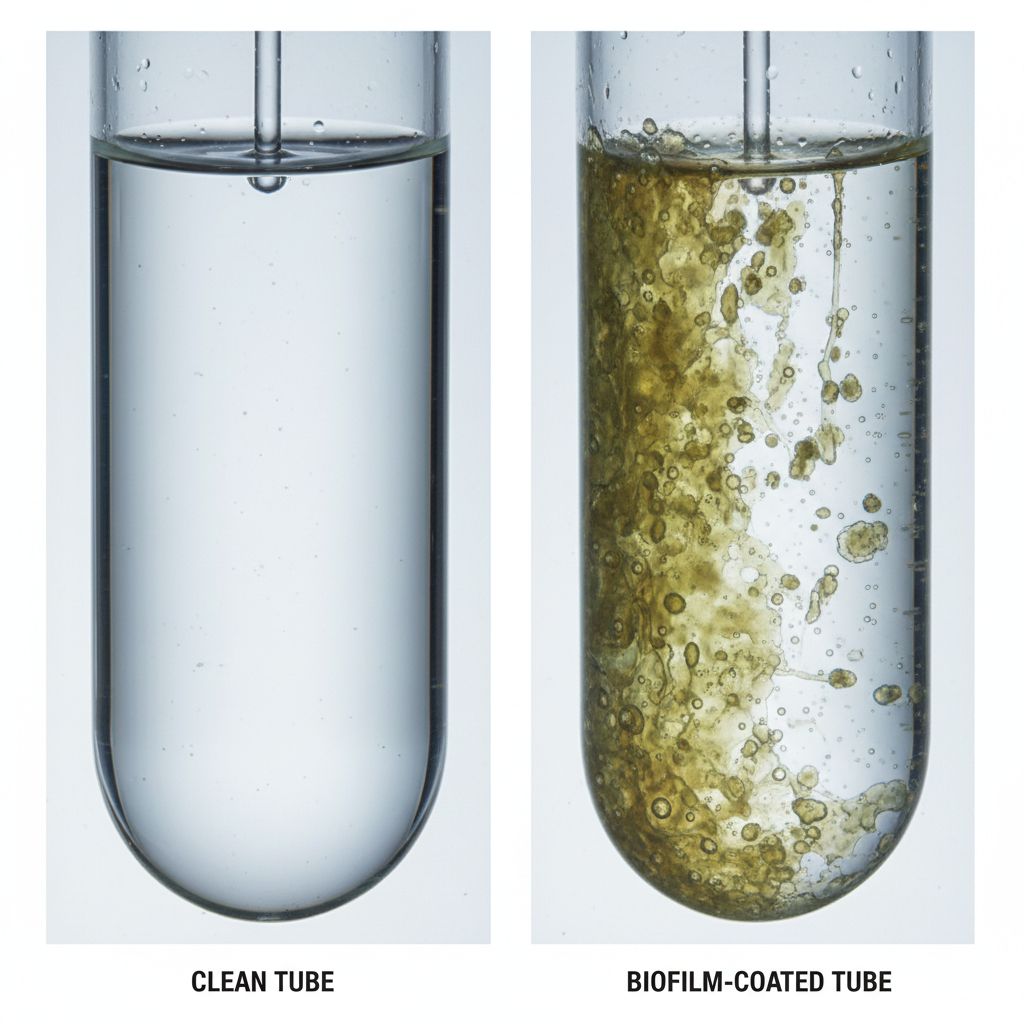
Biofilm is not merely a collection of free-floating microbes; it is a structured community encased in a slimy extracellular polymeric substance (EPS). This matrix shields the embedded microorganisms from disinfectants, making them notoriously difficult to eradicate. The continuous, low-level shedding of bacteria from an established biofilm can lead to water counts far exceeding the standards for safe drinking water, posing a potential risk of infection to patients, especially those who are immunocompromised.
Regulatory bodies worldwide have established stringent guidelines to address this issue. In the United States, the FDA’s Quality System Regulation (21 CFR Part 820) mandates that medical devices be designed and manufactured to prevent contamination. Similarly, standards like ISO 13485:2016 for quality management systems and the EU Medical Device Regulation (MDR) require manufacturers to address infection control throughout the device lifecycle. For dental practices, this translates into a clear responsibility to maintain water quality.
Common Misconceptions vs. Reality
A pervasive myth in waterline maintenance is that occasional “shock” treatments with a high-concentration disinfectant are sufficient to control biofilm. While a shock treatment can temporarily reduce the microbial load, our experience shows that biofilm regrowth can occur within weeks, and sometimes even days, if not supported by a continuous management strategy. Relying solely on periodic shocks is an incomplete solution that fails to address the root cause of contamination.
Effective management requires a layered approach that integrates continuous treatment with regular mechanical and chemical cleaning. This is a core principle behind the design of modern dental chairs, which often incorporate features that simplify and automate this process. For a deeper understanding of how physical design aids cleanliness, exploring how chair design impacts infection control and hygiene provides valuable context.
How Integrated Disinfection Systems Provide a Solution
Modern dental units increasingly feature integrated disinfection systems designed to automate and improve the consistency of waterline maintenance. These systems are engineered to overcome the limitations of manual methods, offering a more reliable and less labor-intensive approach to ensuring water quality.
An integrated system typically includes:
- A Self-Contained Water Reservoir: This isolates the dental unit from municipal water supplies, which can be a source of initial contamination. It allows the practice to control the quality of the source water used.
- A Dosing Mechanism: This component automatically introduces a low-level antimicrobial agent into the water. This continuous treatment helps suppress microbial growth during daily operations, preventing new biofilm from establishing.
- A Control Interface: This allows the dental team to initiate automated cleaning cycles, such as overnight disinfection or intensive shock treatments, with the press of a button.
The Layered Maintenance Protocol in Practice
The true strength of an integrated system is its ability to facilitate a multi-faceted protocol. I have found that the most successful practices move beyond a simple “set it and forget it” mentality and adopt a structured maintenance schedule. This proactive approach not only ensures compliance but also extends the life of dental equipment by preventing buildup and material degradation.
Here is a sample framework that has proven effective in high-utilization clinics:
| Frequency | Action | Purpose & Key Considerations |
|---|---|---|
| Between Patients | Mechanical Flush | Flush all lines (handpieces, syringes) for 20–30 seconds. This simple step expels any contaminants that may have entered the line during the previous procedure. |
| Daily (End of Day) | Air Purge & Flush | Purge all water from the lines with compressed air and/or perform a water flush. This removes stagnant water, a primary contributor to overnight biofilm growth. |
| Weekly | Shock Treatment | Perform a high-concentration disinfection protocol using a chemical compatible with your unit. This eradicates any biofilm that has managed to form despite continuous treatment. In low-use settings, this may be done bi-weekly or monthly. |
| Monthly | Water Quality Monitoring | Use an in-office testing method, such as an ATP meter or heterotrophic plate count (HPC) test strips, to verify water quality. ATP readings consistently above 100 RLU often indicate a failing protocol and the need for an immediate, aggressive shock treatment. Keep a simple log for auditing purposes. |
| Annually | Tubing Inspection/Replacement | Inspect all waterlines for signs of discoloration, cracking, or deposits. Plan for annual replacement of critical tubing, such as handpiece lines, as a preventative measure. |
One of the most common mistakes is using incompatible disinfectants that can cause tubing to swell, become brittle, or degrade over time. Always verify chemical compatibility with the chair manufacturer before introducing a new agent into your protocol.
Wrapping Up: A Commitment to Safety and Reliability
Maintaining the microbial quality of dental unit waterlines is not a one-time task but an ongoing commitment. Biofilm is a resilient adversary, and controlling it demands a systematic, multi-layered strategy. Integrated disinfection systems are a powerful technological ally in this effort, providing the automation and consistency needed for effective, long-term waterline management.
By combining the continuous suppression offered by these systems with a disciplined protocol of mechanical flushing, shock treatments, and regular monitoring, dental practices can operate with confidence. This ensures not only compliance with regulatory standards but, more importantly, the safety and well-being of every patient who sits in the chair. This commitment to operational excellence is the foundation of a trustworthy and reputable practice.
Frequently Asked Questions (FAQ)
1. What is the difference between a shock treatment and continuous treatment?
A shock treatment uses a high concentration of a chemical disinfectant (like bleach or a specialized DUWL cleaner) to kill existing biofilm. It is performed periodically, such as weekly or monthly. Continuous treatment uses a very low, patient-safe dose of an agent (like silver ions or low-concentration hydrogen peroxide) introduced into the waterlines at all times to prevent new biofilm from forming.
2. Can I use tap water in my dental unit’s self-contained bottle?
It is generally not recommended. While it may seem convenient, municipal water can contain microorganisms that will seed the growth of biofilm in your waterlines. Using distilled or sterile water as your source provides a much cleaner starting point.
3. How do I know if my waterline disinfection protocol is working?
The only way to be certain is through regular testing. In-office mail-in test kits or monitoring tools like ATP meters can provide quantitative data on the microbial load in your water, confirming that you are meeting safety standards.
Disclaimer: This article is for informational purposes only and does not constitute professional medical or regulatory advice. Dental professionals should consult with their equipment manufacturer, infection control specialists, and relevant regulatory guidelines to establish a comprehensive waterline maintenance protocol tailored to their specific practice.
References
About the Author





